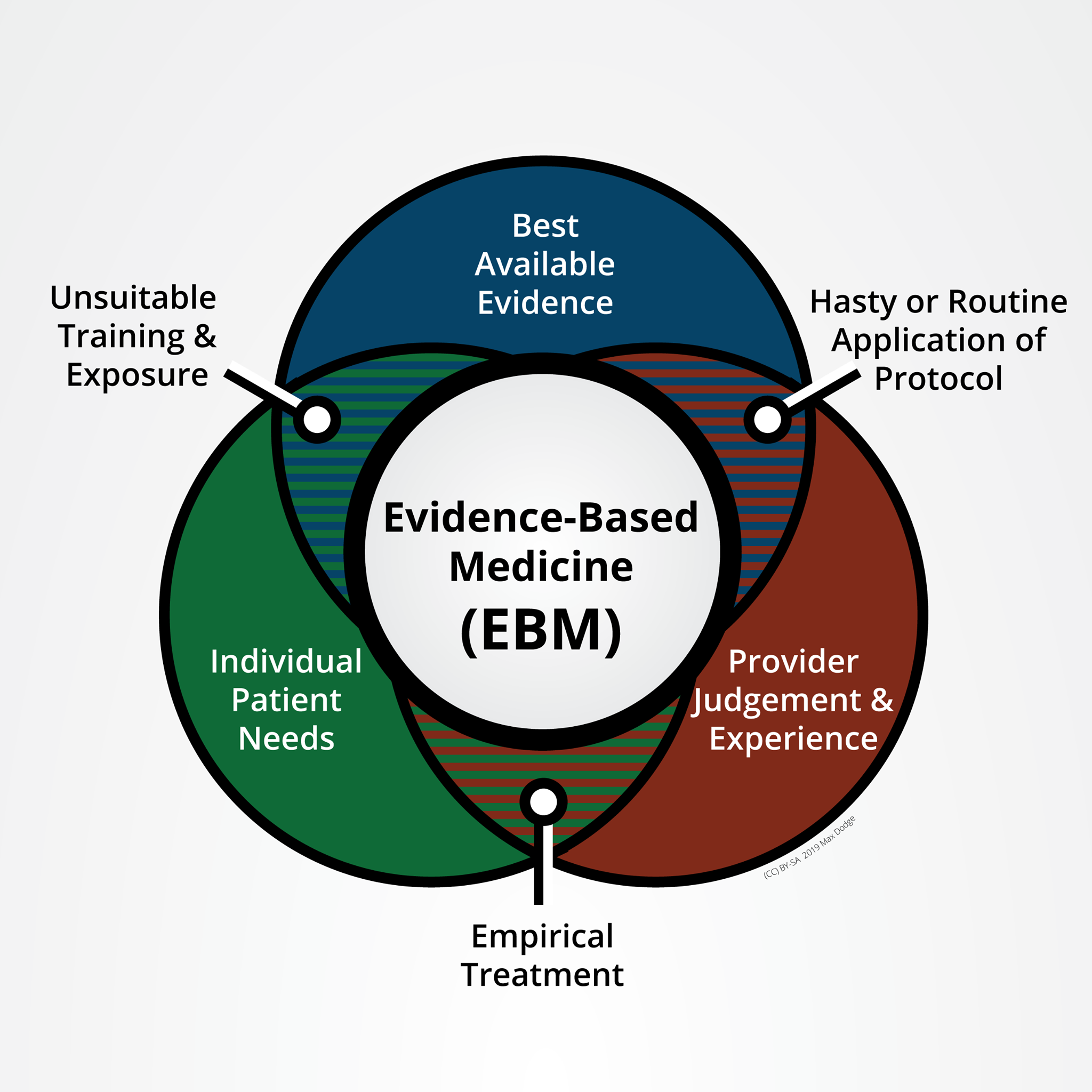
Evidence-Based Medicine (EBM) is the careful, clearly developed, practical, and logical use of modern, best evidence in decision-making about the care of individual patients. EBM relies on three things to be successful:
📚Best Available Evidence gathered through sound scientific practices and carefully evaluated for relevance by all providers.
👩⚕️Provider Judgement & Experience “gestalt” built up through years of successful relevant practice with sufficient volume.
🤒Individual Patient Needs and requirements at hand, whether it’s the specific acute processes of a traumatic injury or the restrictions on care created by someone’s medical history (allergies) or values (religion preventing blood transfusions)
When providers fail to engage all three aspects of the EBM triangle, they create the potential to deliver inappropriate care.
🤷Unsuitable Training & Exposure. Successful providers have access to patient volume, the specific types of patients they expect to treat, and a program that supports development. In the context of trauma, low appropriate patient volume (a rural emergency room), high volume of non-appropriate patients (working in a non-trauma clinic), and programs which don’t emphasize review of appropriate cases all contribute to decreased provider experience and expertise.
🔨Hasty or Routine Application of Protocol. Broadly applying interventions without consideration of the unique aspects of each individual’s situation creates opportunities for inappropriate care. An example would be saying “Any [type] patient will get a [treatment]” Any patient meeting SIRS criteria will get antibiotics and a saline bolus. Any patient with bleeding will get a tourniquet. Hasty treatments are required for perceived life-threatening conditions. Protocols for these events should be based on evidence.
📋Empirical Treatment. Treatment based on the provider’s observations of other similar patients. Observations are a form of evidence and are the beginning of the scientific method but there is much work to be done before a conclusion may be reached. Empirical treatment is educated guesswork.
Key Points:
💊 Journal articles aren’t the end of the EBM cycle, they are one of three essential components.
💊 Learning and development are continual in both knowledge and practice.
“Esse quam videri”